

Coronary Artery Bypass Surgery: Overview
Coronary artery bypass surgery (also known as CABG or “Cabbages” for plural) is considered the gold standard when it comes to treating CAD. This technique was first developed in the Cleveland clinic by Argentinian, Rene Favaloro with several other colleagues in the 1960’s. Basically, the arteries or veins from another part of the victim are retrieved and grafted from the aorta to the coronary arteries, which bypasses the blockage site. In some cases, arteries such as the left internal mammary can be rerouted (instead of completely removed and anastamosed on both ends) to bypass the blockage site and provide blood flow to the heart. The most frequent conduits that are used are the internal mammary arteries, radial arteries, and the saphenous veins (MedicineNet).
CABG Procedure
Preparations
Initially, the operating room is carefully prepared to ensure that all equipments are functioning properly. The patient is brought into the operating room, and transferred onto the operating table. The anesthesiologist inserts various intravenous lines into the patient and injects the anesthesia. After the patient is deemed unconscious, intubation is performed with an endotracheal tube and a metal guide to attach the patient to a mechanical ventilator. Once the endotracheal tube is secured, the mechanical ventilator takes over, and the procedure beings. Throughout the procedure, an anesthesiologist continuously monitors the patient.
Conduit Harvesting
The chest wall is opened by performing a median sternotomy (vertical incision down the sternum) with an cauterizer or a scalpel. Once the sternum is exposed, the surgeon uses an oscillating saw to cut and divide the sternum. After division, a metal separation tool is used to keep the sternum separated. The surgeon then proceeds to observe the heart and surrounding tissue around it. Again, using the cauterizer or scalpel, the surgeon cuts the surrounding tissue to access and expose the left internal mammary artery. When it is sufficiently exposed, the surgeon can determine how the conduits will be used.
Concurrently, a different surgeon usually works on retrieving the saphenous vein from the leg of the patient. Several incisions are made, and once a desired length of the graft is exposed, the surgeon ties both ends with sutures and removes the saphenous vein segment. The segment is placed into a cold saline bath to maintain viability while the surgeon prepares for the heart for the anastamoses.

Cardiac Bypass & Anastamoses
Once the surgeons retrieve the proper conduits, the head surgeon continues the surgery by cutting the pericardium to expose the heart (Figure 7). The heart is examined carefully to determine how the anastamoses will be performed. After proper examination, the surgeon proceeds to connect the cannulas attached to the cardiopulmonary bypass machine, which basically takes over the function of the heart and lungs. In certain cases, off-pump CABG does not require the cardiopulmonary bypass, so the surgeon must perform the CABG with the heart beating continuously throughout the procedure [wikipedia]. The heart is then arrested using several possibilities such as a potassium injection, fibrillation, etc.
Figure 8. A typical CABG with the cannulas placed into the heart.
The cardiopulmonary bypass keeps the blood oxygenated and flowing throughout the body to sustain the patient. Once the heart is arrested, periodic injections of cardioplegia, which is a mixture of various agents to keep the heart
arrested, are directed by the perfusionist controlling the bypass. The surgeon continues the surgery by suturing the graft onto the coronary arteries beyond the blockage sites, while the other end is attached to the aorta or left intact to reroute the blood flow. Once the anastamoses are completed, the surgeon directs the perfusionist to inject blood to test for any leakages. After the leak test, the cannulas are removed and the heart is then restarted. The surgeon ensures that the heart is functioning properly, and then sutures the pericardium shut. A series of thick, pliable wires are then directed in between the ribs to wire the sternum shut. All incisions are closed and covered, and the patient is transferred to the ICU for recovery. The patient is finally monitored in the cardiac surgery ward for several days before release (Wikipedia: Coronary Artery Bypass Surgery).
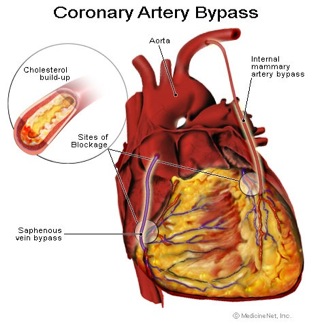
Figure 7. Schematic of a CABG with bypass conduits in place.
